Hi I recently suffered hearing loss in one ear and also tinnitus, ENT doctor thinks a virus. My left ear is good. I’ve been trying a Phonak 90 Lumity life HA. I just can’t get any benefit. I’m a bit concerned that my hearing loss is not the usual type where more amplification helps. If I listen to someone talking through a headphone just through my right ear, I can’t really make out words, its just a crackly noise. If I increase the volume, It’s just a loauder crackly noise. My left ear is fine and does all the work. Could anyone give me some advice? Thank you
1 Like
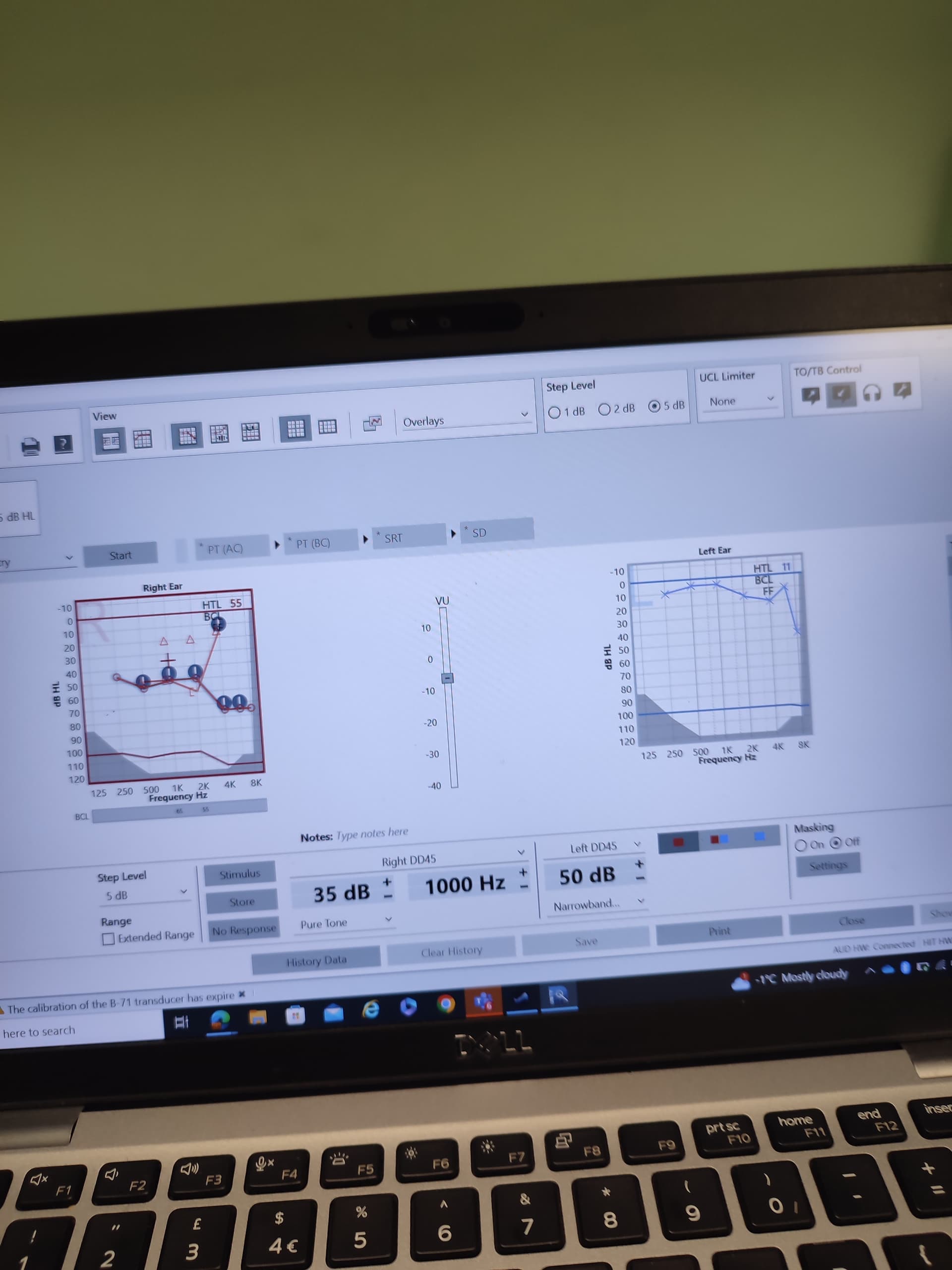
Have you had a hearing test with an audiogram provided to you? That will show your word recognition score for each ear individually. If you post that here, folks can provide better help.
Also has your ENT recommended an mri? That is usually performed to rule out other serious causes of one sided hearing loss. How long ago did this happen to you? I had unilateral hearing loss in my right ear, and for the first month or so I had a LOT of crackling in that ear. That slowly went away. Also my loss changed in that ear over the period of a year. Initially I lost most of the lower frequency. That changed a few times to where the lower frequency came back mostly, and the mid and higher decreased. Each case is unique.
Post your audiogram, or add it to your profile, and also the other info from the audiogram.
CI Candidacy assessment
3 Likes
That cracking sound is similar to my hearing before CI.
The frequencies I heard cracking were dead zones.
Hopefully this is not the case for you.
A CI evaluation will answer a bunch of questions you have about your hearing.
2 Likes
At a guess I would say the Phonak Lumity 90 isn’t the right hearing aid for your profound loss. You may well not find an aid that you can get reasonable hearing in that ear.
As others have suggested a Cochlear Implant might be your best avenue for you to get good hearing in that ear. Speak to your audiologist about the lumity’s not helping with speech recognition. Ask them about a CI evaluation.
Good luck to you.
2 Likes
I was diagnosed with SSNHL. In this case, are hearing aids useless?
2 Likes
@lee1 i had a SSHL my AuD said Phonak Bolero SP. I couldn’t get any sort of clarity with the super power aid at all. (I’m bilateral severe profound). I struggled with them for 18 months I found these to be useless. I moved onto a CI and I’m now bimodal.
You could try the Phonak Naida aid just to see if you get clarity of speech. Also a cross aid might give you clarity. But no guarantees at all. BUT if you try these make sure you take them on trial only so you can return them.
As others have said before a Ci would be your most likely source for success.
Good luck.
3 Likes
It’s possible that with consistent heading aid use, some of the clarity on that ear will return. The loss isn’t that bad. But it sort of depends where you’re starting from. If your current clarity in that ear is <30% I wouldn’t expect miracles. A CI candidacy assessment gives you more information regardless of what choice you make.
3 Likes
CI evaluation is more thorough testing and would give you a full list of options to consider. Would be a shame to invest in a HA and then still feel you are not hearing as well as you could with a CI.
2 Likes
Thank you for your advice. The strange things is that because my other ear is good, there are not many situations where I struggle to hear. In a big restaurant or warehouse I struggle with people talking on my right. All other situations are not a problem, other than this annoying constant tinnitus
1 Like
I would caution that it is tempting to just give up on an ear when there are minimal functional difficulties, but that may not be the case for your entire life and 30 years from now if there’s hearing loss developing in the other ear there may be regrets about just letting the first one go.
1 Like
Are you saying I should try to get the bad ear doing more work because If I don’t it could stop working all together? Thanks
A sudden loss of this magnitude really needs investigation to find the cause. SSNHL is pretty broad, and even includes the catch-all Meniere’s disease. I would think that an ENT should be able to determine absolutely if it’s due to infection. Sometimes they use steroids and see if a missed inflammation can be mitigated. Beyond that, we’re into neurological causes.
In my neurological case, it was an acoustic neuroma (AN). Instant hearing loss, screaming tinnitus, but also vertigo. Only a contrast MRI can make that diagnosis. But it was worse than a simple change in frequency response: We’re talking pitch shifting and scrambling of speech, both of which lasted about 7 years until my auditory center annealed itself to the new condition. No hearing aid could ever solve those problems! I simply had to wait.
Another side-effect of my AN is permanent distortion – and yes I could sometimes describe it as a crackly sound – aggravated by louder sounds and higher pitches. In fact, the hearing aid can and does make this worse in some circumstances, so my equalization and compression have to be carefully adjusted. Having Phonak Target software has been useful to me since I can tweak those parameters.
So my advice is to keep trying to get your docs to look for a root cause, especially if it’s something that could get worse without treatment (if available). I do NOT like mysteries when it comes to my health! With any luck, some or all of this will recover with time. Best of luck to you.
3 Likes
Best of luck and best wishes to you as well, Gary.
1 Like
Thank you for your help. I will try and hurry the MRI appointment up
Yes, basically. Long-term auditory deprivation results in organizational changes in the auditory cortex that can eventually make that ear un-usable. Being a candidate for an implant now does not mean that you will be one forever. I think where I am the limit is 10 years? But the expectation is always that earlier implantation results in better outcomes. Similarly, a trial with a hearing aid is probably worthwhile, but the expectations are the same–if you leave it, the outcomes won’t be as good. Note that it’s not a change in sensitivity that is expected, but a change in clarity/resolution–the expectation isn’t that you will be less able to hear sounds, but that over time your brain will be less able to interpret them. This doesn’t happen so quickly that you should feel like you are in a rush, but on the other hand you also shouldn’t completely ignore it forever.
Try not to worry too much. Acoustic neuroma does need to be ruled out, but they are pretty rare and generally very slow growing and benign. Most people get back a normal MRI and, in the case that there is a neuroma, waiting doesn’t typically change anything for treatment or outcomes. But in all likelihood your sudden loss was a more standard viral neuritis, the event that caused it is over and you are just dealing with the fallout now. The hardest part is waiting to find out. For your own sanity, I suggest (as possible) just assuming that the MRI will be negative.
1 Like
I suffered with a similar condition. If one ear remains good, then I’m not sure that a CI will do much for you.
I had Phonak aids that bounced the sound from my bad side to my good side- this meant that I could hear in social situations rather than struggle with anyone on my ‘bad’ side. This helped considerably.
In time, my good ear went the same way and now I really struggle- but I hope you are a way off that yet! Enjoy your good hearing whilst you can, even though it is frustrating to have a poor side.
1 Like
I mean, it would be the difference between one hearing ear and two hearing ears.
1 Like
Just out of curiosity @Neville… I believe here in the UK, the CI Surgeon will in most instances, opt for the good ear when evaluating a potential Cochlear Implantee, so I was reliably informed? Is this the same in Canada, USA or indeed Australia, I wonder… Or is there a choice? I read somewhere, between a 4% & 10% recorded CI failure rate, and looking at it from an CI candidate perspective, I could accept a failure in my bad ear (there isn’t much residual hearing left) but this might be catastrophic, if the failure was in my good ear… I am aware, the CI Surgeon is going to pick his best option of success, but this isn’t without a certain amount of risk! Your thoughts… Cheers Kev 
1 Like